New Technologies In Dentistry
We live in a time when technology is advancing faster than most of us can keep up. Take our iPhones for instance. They have only been on the market for ten and a half years, and even then…the early models look like bricks compared to the highly sophisticated devices we have in our pockets now.
And to think we sent the first spaceships into orbit with less technology than is in wrist watches today! In the medical setting we have also seen hug leaps in technology in the past few decades. From cancer treatments that use a patient’s own cells to fight tumors to lasers in dentistry that whiten teeth, we live in the best time for medical advancements.
Keep reading as we highlight some of the biggest innovations in dentistry over the past decades!

Highlighting cool technologies in dentistry
Throwing it way back, the discovery of fluoride and the invention of modern toothpaste in the last century revolutionized and changed the course of oral care. Our not-too-distant relatives commonly lost all their teeth in early adulthood and suffered greatly from oral health problems due to the lack of proper hygiene products. The combination of fluoride and modern toothpaste change the course of oral health.
While the idea of dental implants is not new (in fact they date back to 600 A.D.), innovation over the last several decades has brought this ancient idea into the future. Over the last 30 years, dentists and researchers have learned more about how implants can integrate with the jawbone. Today, many experts point to the discovery that titanium can physically bond with living bone tissue as the catalyst to the modernization of dental implants. Modern implants use titanium to form an artificial root of the tooth. Once surgically implanted into the jawbone, the titanium bonds with the jawbone and heals much quicker than previous iterations. This technology brings comfort, aid in eating and confidence to millions of Americans every year.
Another dental technology that has changed the landscape is teeth whitening. Once again, the idea has been around for decades; however, modern technology has allowed patients to have office-quality whitening service at home. Tray whitening has allowed people to complete the treatment at home and new laser-based technology has allowed for quick in-office procedures that give same-day results. In addition to these, over-the-counter products have also become more accessible to the masses.
Onto the future…
In addition to the technologies that are currently dominating the marketplace, there are always new things right around the corner. As dentists, we are always excited to discover new technologies that can make appointments easier for patients and keep their teeth healthy! Ultrasound technology is one budding innovation that allows dentists the option of radiation-free imaging and 3D images of the teeth. There is still work to be done here since the images are not always very crisp. However, there are always new breakthroughs in ultrasound technology and we hope it will eventually be a viable alternative.
3D printing has taken the world (and dentistry world) by storm. A new proprietary method opened by Carbon boasts printing speeds more than 100 times faster than your traditional 3D printer. This technology has already begun to be harnessed by using 3D printers to make dentures! This technology will allow dentists to do things more accurately, faster and cheaper than traditional methods. This all results in more benefits for the patient!
Finally, virtual reality is no longer just for video games. Thanks to its proliferation in the market, virtual reality training is beginning to change the way dentists are trained in dental school and continuing education classes. These systems allow dentists to hone their skills and experiment all without the presence of an actual patient. In addition to the dentists benefitting, some offices are allowing their most anxious patients to wear virtual reality headsets during exams to calm nerves and provide an escape.
Technology is every changing and here at Dr. Ku’s are always keeping our eyes out for new products that can make your trip to the dentist even better!
The post Technology in dentistry appeared first on Fort Worth Dentist | 7th Street District | H. Peter Ku, D.D.S. PA.
Technology in dentistry posted first on http://dentistfortworth.blogspot.com

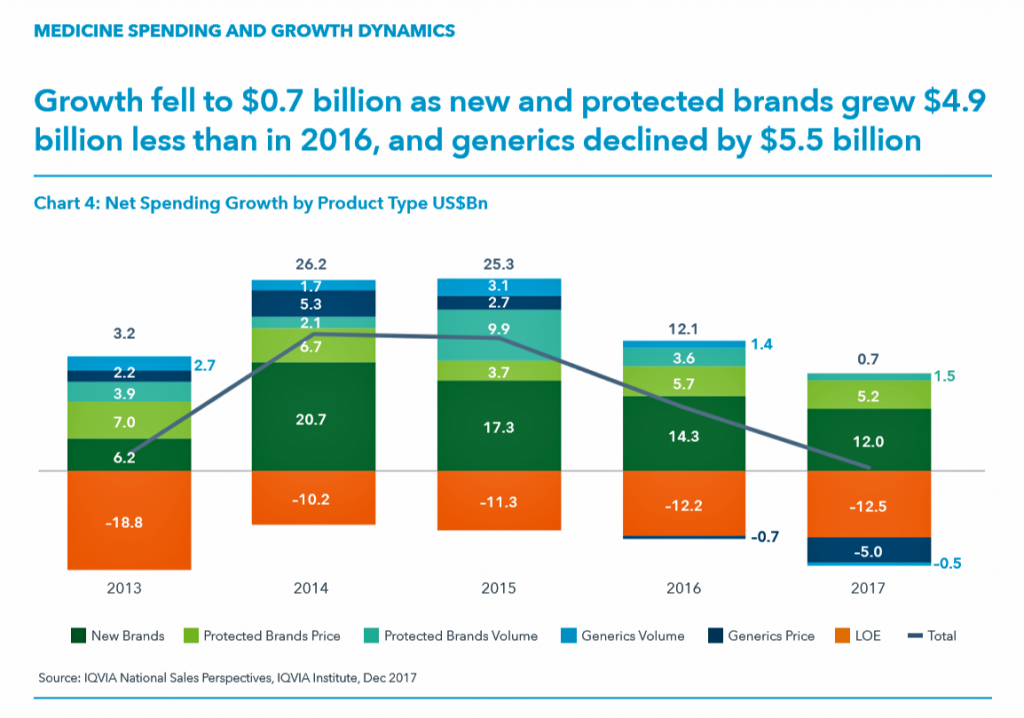

 Health Populi’s Hot Points: As new-new drug therapies come on-stream, prescribers look to trusted information sources beyond the pharma manufacturer of the product for information on use of the new medicine.
Health Populi’s Hot Points: As new-new drug therapies come on-stream, prescribers look to trusted information sources beyond the pharma manufacturer of the product for information on use of the new medicine. 
 As the nation battles an obesity epidemic that adds $$ costs to U.S. national health spending, there are many opportunities to address this impactful social determinant of health to reduce health spending per person and to drive public and individual health. In this post, I examine a few very current events in the food-as-medicine marketspace.
As the nation battles an obesity epidemic that adds $$ costs to U.S. national health spending, there are many opportunities to address this impactful social determinant of health to reduce health spending per person and to drive public and individual health. In this post, I examine a few very current events in the food-as-medicine marketspace.
 Once Upon A Farm works with partner farms on the U.S. west coast, positioning the baby-and-toddler foods as nutrient-dense without preservatives, concentrates or processed purees — “delivered fresh from farm to highchair
Once Upon A Farm works with partner farms on the U.S. west coast, positioning the baby-and-toddler foods as nutrient-dense without preservatives, concentrates or processed purees — “delivered fresh from farm to highchair ,” their tagline asserts.
,” their tagline asserts. Health Populi’s Hot Points: One of the long-missing pieces of this food-health puzzle has been medical education. “He knew the dearth of nutrition training in medical schools was a problem that went far beyond his experience. Five years ago, he left his university-based cardiology practice in Chicago to launch the Gaples Institute for Integrative Cardiology in Deerfield, Illinois, a nonprofit that aims to improve nutrition and lifestyle education for health care professionals,”
Health Populi’s Hot Points: One of the long-missing pieces of this food-health puzzle has been medical education. “He knew the dearth of nutrition training in medical schools was a problem that went far beyond his experience. Five years ago, he left his university-based cardiology practice in Chicago to launch the Gaples Institute for Integrative Cardiology in Deerfield, Illinois, a nonprofit that aims to improve nutrition and lifestyle education for health care professionals,”  We come full circle and return to the B Corps Declaration of Interdependence, which reads:
We come full circle and return to the B Corps Declaration of Interdependence, which reads: Walmart has been a health/care destination for many years. The company that defined Big Box stores in their infancy grew in healthcare, health and wellness over the past two decades, pioneering
Walmart has been a health/care destination for many years. The company that defined Big Box stores in their infancy grew in healthcare, health and wellness over the past two decades, pioneering  Health Populi’s Hot Points: I recently spoke at a meeting in Bentonville about Walmart as a front-door to health for the new patient-as-payor. From the pharmacy to health-and-beauty (THINK: headaches, vitamins and supplements, and good skin care), the grocery (for food-as-medicine and healthy eating for families), vision and oral care (often overlooked since the Great Recession of 2008), the urgent care Clinic at Walmartand primary care doctor access in the Care Clinic, and Walmart’s “biggest health fairs” convened throughout the year.
Health Populi’s Hot Points: I recently spoke at a meeting in Bentonville about Walmart as a front-door to health for the new patient-as-payor. From the pharmacy to health-and-beauty (THINK: headaches, vitamins and supplements, and good skin care), the grocery (for food-as-medicine and healthy eating for families), vision and oral care (often overlooked since the Great Recession of 2008), the urgent care Clinic at Walmartand primary care doctor access in the Care Clinic, and Walmart’s “biggest health fairs” convened throughout the year.

 The second chart covers years lived with disability — the quality of life stuff, like pain which dominates the list via low back, migraine, and neck. Depression and mental/behavioral health conditions also feature prominently in years lived with disability.
The second chart covers years lived with disability — the quality of life stuff, like pain which dominates the list via low back, migraine, and neck. Depression and mental/behavioral health conditions also feature prominently in years lived with disability. The evidence in terms of outcomes and the burden of disease by US state demonstrates, “no,” we do not.
The evidence in terms of outcomes and the burden of disease by US state demonstrates, “no,” we do not.
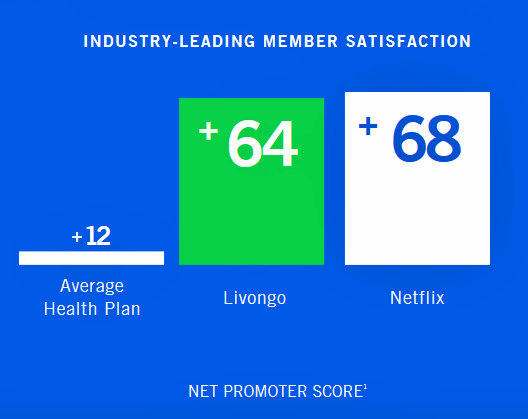 That human-centered design approach is evident in Livongo’s net promoter scores gifted by consumers. Note the member satisfaction bar chart, illustrating that Livongo scores nearly as high as Netflix. The average health plan fetches a low +12 points, with Livongo scoring five times greater engagement. I noted the dismal consumer experience ratings of health plans earlier this week covering the
That human-centered design approach is evident in Livongo’s net promoter scores gifted by consumers. Note the member satisfaction bar chart, illustrating that Livongo scores nearly as high as Netflix. The average health plan fetches a low +12 points, with Livongo scoring five times greater engagement. I noted the dismal consumer experience ratings of health plans earlier this week covering the  Note the third graphic, illustrating the growing costs of healthcare in America relative to other spending line items in the Federal budget. Health care is crowding out other priorities, like education, environment, and transportation infrastructure — all key to a healthy future for citizens — morphing into health citizens.
Note the third graphic, illustrating the growing costs of healthcare in America relative to other spending line items in the Federal budget. Health care is crowding out other priorities, like education, environment, and transportation infrastructure — all key to a healthy future for citizens — morphing into health citizens. he concept of patients accessing EHRs is a health behavior change challenge: 63% of physicians whose providers encouraged them to look at the EHR did so; only 38% of patients with providers that did not encourage EHR access looked at their records.
he concept of patients accessing EHRs is a health behavior change challenge: 63% of physicians whose providers encouraged them to look at the EHR did so; only 38% of patients with providers that did not encourage EHR access looked at their records. Health Populi’s Hot Points: Designing for patient experience, that is user/consumer experience (UX/CX), is a key to inspiring people to engage in their health, which
Health Populi’s Hot Points: Designing for patient experience, that is user/consumer experience (UX/CX), is a key to inspiring people to engage in their health, which 

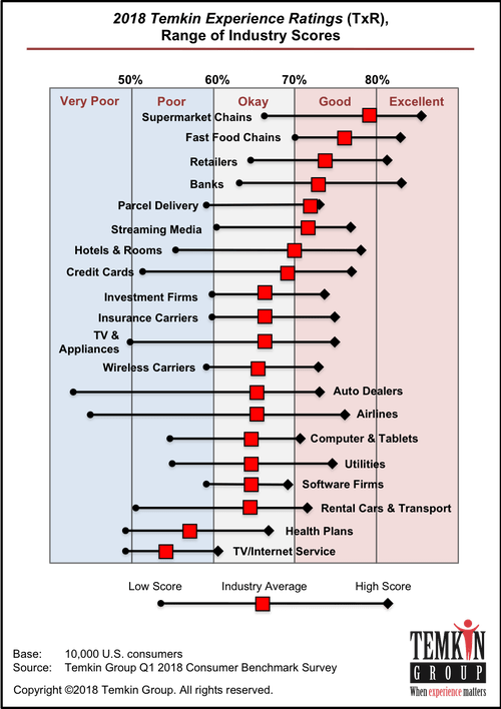 U.S. consumers rank supermarkets, fast food chains, retailers, and banks as their top performing industries for experience according to the
U.S. consumers rank supermarkets, fast food chains, retailers, and banks as their top performing industries for experience according to the